Appropriations committee hears overview of Vermont’s Rural Health Transformation program
March 10, 2026 | Appropriations, HOUSE OF REPRESENTATIVES, Committees, Legislative , Vermont
This article was created by AI summarizing key points discussed. AI makes mistakes, so for full details and context, please refer to the video of the full meeting. Please report any errors so we can fix them. Report an error »
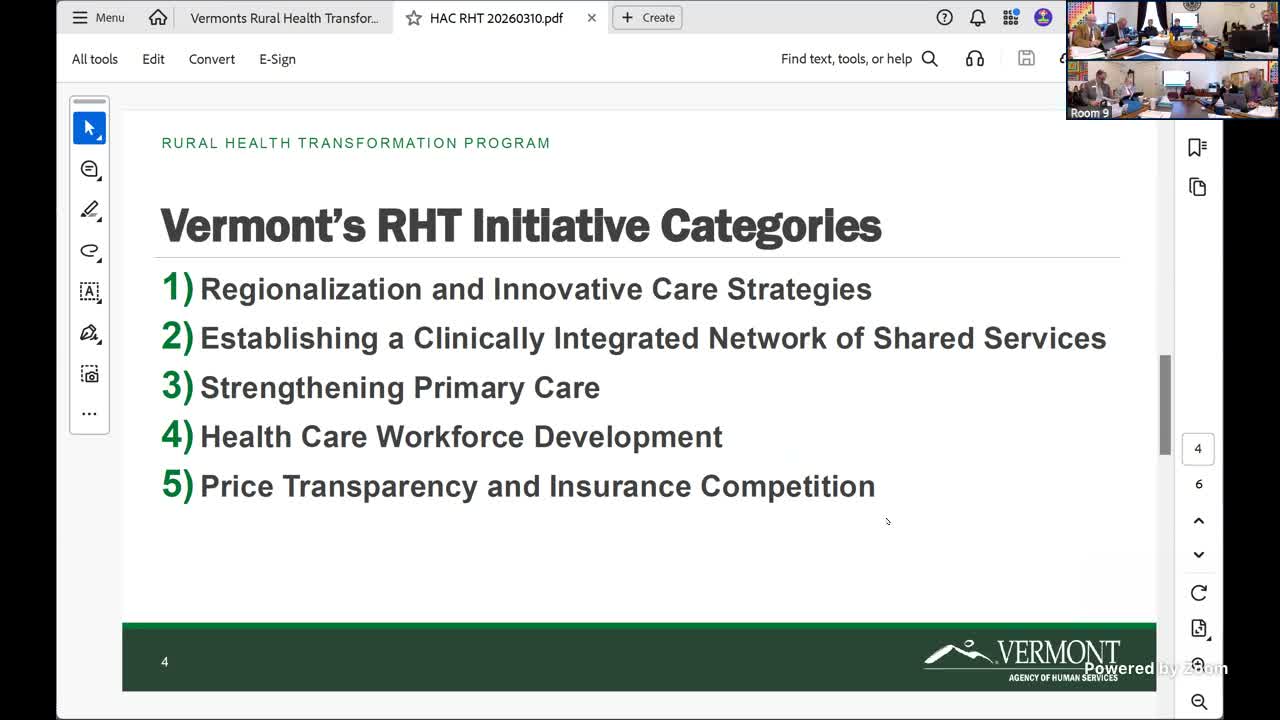
The House Appropriations Committee on March 10 heard a broad overview of Vermont’s Rural Health Transformation (RHT) program, which the presenter said groups projects into regionalization, shared services, primary care modernization and workforce initiatives and will prioritize awards that require the longest procurement timelines.
The presentation from the program lead (identified in the hearing as Jill) laid out the team’s approach to obligating federal funds and to sequencing grant and contract solicitations. “August 1 is our sort of internal deadline for obligating the funds,” Jill told the committee, underscoring the timeline driving prioritization decisions. She added that “I believe the very first RFP was released this week, and it's gonna be blown up on our website,” and that the program will use a listserv and weekly announcements so providers do not have to constantly refresh the site for opportunities.
Nut graf: Why this matters — RHT is intended to shift some health-care services from hospital‑centric models to community and regional approaches, expand access in rural areas and invest one‑time federal dollars where they can be sustained or transitioned into longer‑term payment arrangements. The briefing outlined concrete project types that will be funded and the constraints that shape which solicitations the state can issue now versus later.
Jill walked the committee through the major project buckets. Under regionalization, the first seven projects focus on making certain services available either locally, regionally or statewide; examples include community paramedicine pilots that expand EMS roles to provide in‑home care and high‑acuity equipment in nursing homes such as dialysis and ventilators. On facility upgrades she cautioned there is a federal cap: “The cap is pretty high. It’s I actually can’t think of it now, but it's I think it's higher than the provider payment cap,” and said the program consolidated facility upgrades into a single bucket to avoid confusion about separate dollar limits.
The shared‑services bucket includes back‑office systems such as shared human‑resources platforms and shared electronic medical records to improve interoperability, plus statewide eConsult tools that would let rural clinicians consult specialists. The primary‑care bucket covers capacity payments to practices for longer hours, care coordinators and behavioral‑health integration; some payment‑model dollars have been released by CMS while other payment models remain under development.
Jill also described workforce investments — conditional tuition assistance with a five‑year work commitment, residency programs to help new graduates enter home‑based care, and targeted training — and said some grants will be structured as subrecipient awards while other work will be procured through contractors following state procurement rules. She added the program will hire an independent evaluator and fund analytics to inform transformation decisions.
The presenter warned that several buckets remain constrained by CMS approvals: “They have not released these dollars yet. We're not authorized to do an RFP,” she said, referring to certain transformation‑integration funds that still require more detail for CMS to authorize release. Committee members asked how these constraints and caps will interact with existing regulatory approvals; Jill replied that existing regulatory frameworks still apply and that program funding does not change those requirements.
The briefing also touched on sustainment: the presenter said sustainability is an explicit goal and that the state is thinking about transition paths if federal models (such as AHEAD or Medicare participation) can be aligned with the work. She cautioned that closing services without careful planning can risk capacity shortages and said the program will use analytics and technical assistance to guide decisions.
The committee requested additional detail on specific projects and the presenter invited members to follow up offline. The presenter said staffing is underway: a finance manager position has been filled and a project manager hire is imminent. The committee scheduled to reconvene at 1 p.m. to consider other business, including bill 67.
Ending: The briefing provided a roadmap of projects and a clear timeline constraint for obligating funds, while leaving several CMS‑dependent buckets and many operational details to be resolved through forthcoming RFPs and procurement work. The committee said it will follow up for deeper detail on specific projects.
The presentation from the program lead (identified in the hearing as Jill) laid out the team’s approach to obligating federal funds and to sequencing grant and contract solicitations. “August 1 is our sort of internal deadline for obligating the funds,” Jill told the committee, underscoring the timeline driving prioritization decisions. She added that “I believe the very first RFP was released this week, and it's gonna be blown up on our website,” and that the program will use a listserv and weekly announcements so providers do not have to constantly refresh the site for opportunities.
Nut graf: Why this matters — RHT is intended to shift some health-care services from hospital‑centric models to community and regional approaches, expand access in rural areas and invest one‑time federal dollars where they can be sustained or transitioned into longer‑term payment arrangements. The briefing outlined concrete project types that will be funded and the constraints that shape which solicitations the state can issue now versus later.
Jill walked the committee through the major project buckets. Under regionalization, the first seven projects focus on making certain services available either locally, regionally or statewide; examples include community paramedicine pilots that expand EMS roles to provide in‑home care and high‑acuity equipment in nursing homes such as dialysis and ventilators. On facility upgrades she cautioned there is a federal cap: “The cap is pretty high. It’s I actually can’t think of it now, but it's I think it's higher than the provider payment cap,” and said the program consolidated facility upgrades into a single bucket to avoid confusion about separate dollar limits.
The shared‑services bucket includes back‑office systems such as shared human‑resources platforms and shared electronic medical records to improve interoperability, plus statewide eConsult tools that would let rural clinicians consult specialists. The primary‑care bucket covers capacity payments to practices for longer hours, care coordinators and behavioral‑health integration; some payment‑model dollars have been released by CMS while other payment models remain under development.
Jill also described workforce investments — conditional tuition assistance with a five‑year work commitment, residency programs to help new graduates enter home‑based care, and targeted training — and said some grants will be structured as subrecipient awards while other work will be procured through contractors following state procurement rules. She added the program will hire an independent evaluator and fund analytics to inform transformation decisions.
The presenter warned that several buckets remain constrained by CMS approvals: “They have not released these dollars yet. We're not authorized to do an RFP,” she said, referring to certain transformation‑integration funds that still require more detail for CMS to authorize release. Committee members asked how these constraints and caps will interact with existing regulatory approvals; Jill replied that existing regulatory frameworks still apply and that program funding does not change those requirements.
The briefing also touched on sustainment: the presenter said sustainability is an explicit goal and that the state is thinking about transition paths if federal models (such as AHEAD or Medicare participation) can be aligned with the work. She cautioned that closing services without careful planning can risk capacity shortages and said the program will use analytics and technical assistance to guide decisions.
The committee requested additional detail on specific projects and the presenter invited members to follow up offline. The presenter said staffing is underway: a finance manager position has been filled and a project manager hire is imminent. The committee scheduled to reconvene at 1 p.m. to consider other business, including bill 67.
Ending: The briefing provided a roadmap of projects and a clear timeline constraint for obligating funds, while leaving several CMS‑dependent buckets and many operational details to be resolved through forthcoming RFPs and procurement work. The committee said it will follow up for deeper detail on specific projects.
View the Full Meeting & All Its Details
This article offers just a summary. Unlock complete video, transcripts, and insights as a Founder Member.
✓
Watch full, unedited meeting videos
✓
Search every word spoken in unlimited transcripts
✓
AI summaries & real-time alerts (all government levels)
✓
Permanent access to expanding government content
30-day money-back guarantee
