FAA updates AME guidance on valve disease, atrial flutter, carotid stenosis and coronary imaging
February 27, 2026 | Federal Aviation Administration (FAA), Department of Transportation (DOT), Executive, Federal
This article was created by AI summarizing key points discussed. AI makes mistakes, so for full details and context, please refer to the video of the full meeting. Please report any errors so we can fix them. Report an error »
Federal Aviation Administration medical officers announced several cardiovascular updates to the AME (Aviation Medical Examiner) guide during the agency’s January Grand Rounds, clarifying when examiners should issue medical certificates, seek special issuance and defer cases to FAA review.
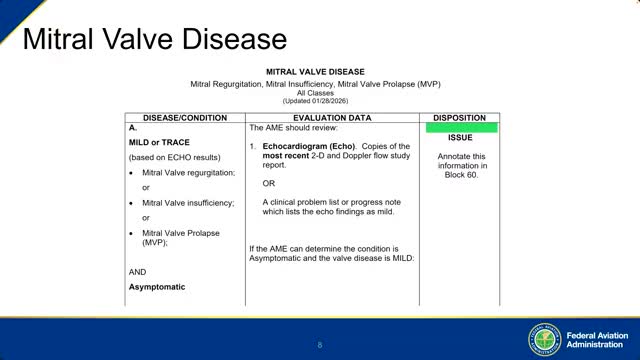
Dr. Greg Bindrick, a medical officer and physician trainer at the Civil Aerospace Medical Institute, described the new disposition rules for mitral valve disease: mild or trace disease with no symptoms remains eligible for routine issuance after the AME uploads the echo; moderate cases generally proceed to special issuance and require a current echocardiogram plus a detailed cardiology progress note; severe disease is likely to be denied until the aeromedical risk is mitigated by intervention such as valve repair or replacement.
"If it's moderate, it's most likely usually gonna be a special issuance," Bindrick said, advising AMEs to obtain cardiology interpretation and to consider 24-hour Holter monitoring when moderate-to-severe regurgitation is present.
The FAA also described a distinct pathway for "typical" atrial flutter treated with ablation. Bindrick said that if ablation occurred more than two years earlier, and the pilot is asymptomatic and off antiarrhythmic medications, the AME should obtain a cardiology-completed status summary form and may proceed with routine issuance. If the ablation was less than two years ago, the AME should defer, submit the procedure report and a cardiology DCPN, and obtain Holter monitoring performed no sooner than 90 days after ablation for FAA review.
Bindrick introduced a khaki worksheet for asymptomatic carotid or vertebral artery stenosis. Under the guidance, stenosis less than 50 percent is compatible with regular issuance provided there are no symptoms and no anticoagulation; the 50–79 percent range (reported as less than 80 percent) may qualify for the khaki pathway with current imaging and clinical notes; stenosis of 80 percent or greater, anticoagulation, a history of TIA or stroke, or a treating physician recommending surgery remove the case from the khaki pathway and require full FAA consideration.
The session included substantial detail on coronary calcium scores and coronary CT angiography. For first- or second-class pilots, the FAA requires an invasive cardiac catheterization when the calcium score exceeds 400. A coronary CTA will be accepted only if accompanied by CT-derived fractional flow reserve (CT-FFR); Bindrick emphasized that CT-FFR is not universally available and often carries an out-of-pocket fee. Scores from 101 to 400 generally require a nuclear (radionuclide) stress test; scores of 100 or below are typically acceptable for issuance.
"If they're a first or second class pilot and their calcium score is over 400, we really, really want a cardiac cath," Bindrick said, adding that an invasive cath can also allow immediate treatment such as stent placement.
Bindrick noted FAA will continue to follow pilots with nonobstructive CT-FFR or after cath under special issuance protocols and may require periodic testing as appropriate. He urged AMEs to upload exam reports to the applicant’s record and to note key items in block 60 so FAA reviewers can access documentation.
The FAA said these changes are being incorporated into the AME guide; Bindrick told attendees the guidance had been added to the guide as of that afternoon and that AMEs should follow the updated worksheets and status summaries going forward.
The session ended with an invitation for AMEs to submit suggestions to the AME guide team via ameguide@fa.gov and a reminder that FAA staff would remain in a debrief breakout room.
Dr. Greg Bindrick, a medical officer and physician trainer at the Civil Aerospace Medical Institute, described the new disposition rules for mitral valve disease: mild or trace disease with no symptoms remains eligible for routine issuance after the AME uploads the echo; moderate cases generally proceed to special issuance and require a current echocardiogram plus a detailed cardiology progress note; severe disease is likely to be denied until the aeromedical risk is mitigated by intervention such as valve repair or replacement.
"If it's moderate, it's most likely usually gonna be a special issuance," Bindrick said, advising AMEs to obtain cardiology interpretation and to consider 24-hour Holter monitoring when moderate-to-severe regurgitation is present.
The FAA also described a distinct pathway for "typical" atrial flutter treated with ablation. Bindrick said that if ablation occurred more than two years earlier, and the pilot is asymptomatic and off antiarrhythmic medications, the AME should obtain a cardiology-completed status summary form and may proceed with routine issuance. If the ablation was less than two years ago, the AME should defer, submit the procedure report and a cardiology DCPN, and obtain Holter monitoring performed no sooner than 90 days after ablation for FAA review.
Bindrick introduced a khaki worksheet for asymptomatic carotid or vertebral artery stenosis. Under the guidance, stenosis less than 50 percent is compatible with regular issuance provided there are no symptoms and no anticoagulation; the 50–79 percent range (reported as less than 80 percent) may qualify for the khaki pathway with current imaging and clinical notes; stenosis of 80 percent or greater, anticoagulation, a history of TIA or stroke, or a treating physician recommending surgery remove the case from the khaki pathway and require full FAA consideration.
The session included substantial detail on coronary calcium scores and coronary CT angiography. For first- or second-class pilots, the FAA requires an invasive cardiac catheterization when the calcium score exceeds 400. A coronary CTA will be accepted only if accompanied by CT-derived fractional flow reserve (CT-FFR); Bindrick emphasized that CT-FFR is not universally available and often carries an out-of-pocket fee. Scores from 101 to 400 generally require a nuclear (radionuclide) stress test; scores of 100 or below are typically acceptable for issuance.
"If they're a first or second class pilot and their calcium score is over 400, we really, really want a cardiac cath," Bindrick said, adding that an invasive cath can also allow immediate treatment such as stent placement.
Bindrick noted FAA will continue to follow pilots with nonobstructive CT-FFR or after cath under special issuance protocols and may require periodic testing as appropriate. He urged AMEs to upload exam reports to the applicant’s record and to note key items in block 60 so FAA reviewers can access documentation.
The FAA said these changes are being incorporated into the AME guide; Bindrick told attendees the guidance had been added to the guide as of that afternoon and that AMEs should follow the updated worksheets and status summaries going forward.
The session ended with an invitation for AMEs to submit suggestions to the AME guide team via ameguide@fa.gov and a reminder that FAA staff would remain in a debrief breakout room.
Don't Miss a Word: See the Full Meeting!
Go beyond summaries. Unlock every video, transcript, and key insight with a Founder Membership.
✓
Get instant access to full meeting videos
✓
Search and clip any phrase from complete transcripts
✓
Receive AI-powered summaries & custom alerts
✓
Enjoy lifetime, unrestricted access to government data
30-day money-back guarantee
